This web page was produced as an assignment for Genetics 677, and undergraduate course at UW-Madison.
What is long QT Syndrome?

Imagine living the life of a child where you cannot run around playing tag with your friends or where the sudden buzzing of an alarm clock can put your life at risk. Or imagine being the parent that has to tell their child they cannot participate in strenuous competitive sports for fear that the play might be their last. This is the constant daily life of someone with long QT syndrome, or LQTS
But what is LQTS?
“LQTS is a disorder of cardiac repolarization resulting in QT prolongation on an electrocardiogram.”[4] Unless of course you are a cardiologist or a med student a lot more questions were formed then what were answered, in a more simplified version LQTs is a disorder that causes a malfunctioning of the heart, and it is this malfunctioning that can cause the person to have a sudden loss of consciousness, seizures, or sudden death. [4] We will go into more detail of the malfunctioning of the heart a little further down. This malfunctioning of the heart which may not be seen by the person, family, or doctor until it is to late can be effected by many things, but most of the time when an attack is triggered it is because of an external stimulus such as exercise or a sudden loud noise. Let’s take a more in depth look at the real malfunctioning of the heart.
What is malfunctioning?
In order for a normal heart to fulfill its daily cardiac function there must be a careful balance of phases with specific ion channels opened and closed according to time- and voltage-gated regulation. [1] This movie gives an insight as to how a normal heart functions and sends
the impulses through the cells to contract to create the beat of the heart. However, in people that have LQTS, and more specifically, LQT1, there is a loss-of-function mutation in the gene KCNQ1 which encodes Iks, an adrenergic-sensitive potassium current in the heart. [2] Again to you and me this is just a bunch of big words thrown into a sentence, so let us see if we can change it in a way were you and I can understand it. In a person born with LQTS that person is said to have a disturbance in their heart’s electrical system. In a normal heart, ions (such as potassium, sodium, and chloride) pass into and out of the cell through ion channels in the cell membrane. This transport of ions across the membrane causes electrical activity (depolarization or repolarization), and it is this electrical activity that kicks the mechanical activity of the heart (contraction and relaxation) into gear. These electrical signals can be picked up by a machine and documented on paper. This is called an electrocardiogram, or ECG. This is the paper a cardiologist will look at when determining if someone has LQTS or not. The difference in someone that has LQTS compared to someone who does not is that someone with LQTS has abnormalities in the ion channels that channel potassium and sodium ions into and out of the cell. This can result in a delayed repolarization which in turn leads to the heart beating slower. This will show up on an ECG as a prolonged QT interval. All that the QT stands for is that it is the time interval that encompasses the total time it takes the cells to depolarize and subsequently repolarize. [1] The longer the interval is the longer it takes the heart to recover before being able to beat again, hence why the symptoms of LQTS usually only appear during times when the heart is beating faster than usual.
How does someone get LQTS?
A person can obtain LQTS in two different ways. First the person could have acquired LQTS which usually means that their LQTS symptoms
could be caused by anything that can alter the ion flow through the channels from ion imbalance to unhealthy nutritional states to an indocrine disorder. [4] Unfortunately, the most commonly seen cause of acquired LQTS is through drug use. The other type of LQTS is called congenital LQTS. It is this form of LQTS that is caused by the loss-of-function mutation in the KCNQ1 gene,
and the one that is seen throughout the rest of this
website.
But what is LQTS?
“LQTS is a disorder of cardiac repolarization resulting in QT prolongation on an electrocardiogram.”[4] Unless of course you are a cardiologist or a med student a lot more questions were formed then what were answered, in a more simplified version LQTs is a disorder that causes a malfunctioning of the heart, and it is this malfunctioning that can cause the person to have a sudden loss of consciousness, seizures, or sudden death. [4] We will go into more detail of the malfunctioning of the heart a little further down. This malfunctioning of the heart which may not be seen by the person, family, or doctor until it is to late can be effected by many things, but most of the time when an attack is triggered it is because of an external stimulus such as exercise or a sudden loud noise. Let’s take a more in depth look at the real malfunctioning of the heart.
What is malfunctioning?
In order for a normal heart to fulfill its daily cardiac function there must be a careful balance of phases with specific ion channels opened and closed according to time- and voltage-gated regulation. [1] This movie gives an insight as to how a normal heart functions and sends
the impulses through the cells to contract to create the beat of the heart. However, in people that have LQTS, and more specifically, LQT1, there is a loss-of-function mutation in the gene KCNQ1 which encodes Iks, an adrenergic-sensitive potassium current in the heart. [2] Again to you and me this is just a bunch of big words thrown into a sentence, so let us see if we can change it in a way were you and I can understand it. In a person born with LQTS that person is said to have a disturbance in their heart’s electrical system. In a normal heart, ions (such as potassium, sodium, and chloride) pass into and out of the cell through ion channels in the cell membrane. This transport of ions across the membrane causes electrical activity (depolarization or repolarization), and it is this electrical activity that kicks the mechanical activity of the heart (contraction and relaxation) into gear. These electrical signals can be picked up by a machine and documented on paper. This is called an electrocardiogram, or ECG. This is the paper a cardiologist will look at when determining if someone has LQTS or not. The difference in someone that has LQTS compared to someone who does not is that someone with LQTS has abnormalities in the ion channels that channel potassium and sodium ions into and out of the cell. This can result in a delayed repolarization which in turn leads to the heart beating slower. This will show up on an ECG as a prolonged QT interval. All that the QT stands for is that it is the time interval that encompasses the total time it takes the cells to depolarize and subsequently repolarize. [1] The longer the interval is the longer it takes the heart to recover before being able to beat again, hence why the symptoms of LQTS usually only appear during times when the heart is beating faster than usual.
How does someone get LQTS?
A person can obtain LQTS in two different ways. First the person could have acquired LQTS which usually means that their LQTS symptoms
could be caused by anything that can alter the ion flow through the channels from ion imbalance to unhealthy nutritional states to an indocrine disorder. [4] Unfortunately, the most commonly seen cause of acquired LQTS is through drug use. The other type of LQTS is called congenital LQTS. It is this form of LQTS that is caused by the loss-of-function mutation in the KCNQ1 gene,
and the one that is seen throughout the rest of this
website.
KCNQ1
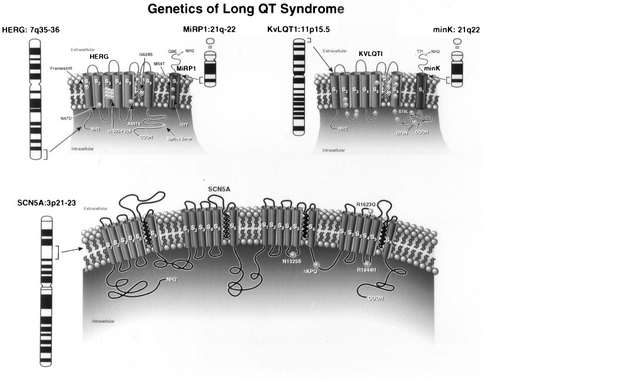
KCNQ1, whose full name is Potassium Voltage-Gated Channel, KQT-like subfamily, member 1, is the gene that many scientists believe is the main cause behind LQTS. Initially called KVLQT1, the gene was found to be a novel potassium channel gene, and after further studies was later renamed to KCNQ1. [3] Spanning roughly 400 kilobases the gene exits of 16 exons and is widely expressed in many of our organs including the heart, lung, kidney, inner ear, placenta, and pancreas, but nt in skeletal muscle, liver, or the brain. [3] The figure to the left illustrates what a normal protein coded for by the KCNQ1 gene should look like. The protein exists as a 6 membrane spanning protein with a core potassium-selective, pore-signature sequence in the middle. Today scientists have found that even if there is no mutation to the KCNQ1 gene it still requires a β-subunit in order to function properly, this β-subunit is referred to as KCNE1 and is a short protein that coassembles with the larger KCNQ1 α-subunit. [3]
References
[1]Kramer, Daniel B and Peter J. Zimetbaum. Long-QT Syndrome. Cardiology in Review. September/October 2011. Vol 19, No 5. DOI: 10.1097/CRD.0b013e3182203504
[2]Roden, Dan M. Long-QT Syndrome. The New England Journal of Medicine. January 2008. http://www.nejm.org.ezproxy.library.wisc.edu/doi/full/10.1056/NEJMcp0706513
[3]Towbin, Jeffrey A. et al. Genotype and Severity of Long QT Syndrome. Drug Metabolism and Disorder. April 2001. Vol 29, No 4. http://dmd.aspetjournals.org
[4]Twedell, Diane Associate Editor. An Overview of Congenital Long QT Syndrome. The Journal of Continuing Education in Nursing.January/February 2005. Vol 36, No 1.
[5] Picture http://t2.gstatic.com/images?q=tbn:ANd9GcRsYSZWoLIB5BJ-0UDKpesgs7pxrgtDBOJ9Oz0OOlkW4KI-4QwBhxDjm5oGCA
[2]Roden, Dan M. Long-QT Syndrome. The New England Journal of Medicine. January 2008. http://www.nejm.org.ezproxy.library.wisc.edu/doi/full/10.1056/NEJMcp0706513
[3]Towbin, Jeffrey A. et al. Genotype and Severity of Long QT Syndrome. Drug Metabolism and Disorder. April 2001. Vol 29, No 4. http://dmd.aspetjournals.org
[4]Twedell, Diane Associate Editor. An Overview of Congenital Long QT Syndrome. The Journal of Continuing Education in Nursing.January/February 2005. Vol 36, No 1.
[5] Picture http://t2.gstatic.com/images?q=tbn:ANd9GcRsYSZWoLIB5BJ-0UDKpesgs7pxrgtDBOJ9Oz0OOlkW4KI-4QwBhxDjm5oGCA
